
Question:
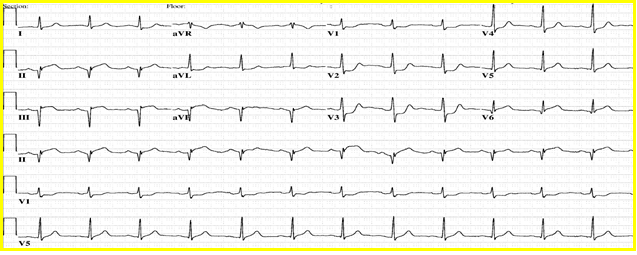
A 59-year old man presents with acute onset shortness of breath, nausea and vomiting, how would you interpret his EKG?
Answer:
The rhythm is sinus. There are Q-waves in the inferior leads with hint of ST elevation in lead III. Most important finding is dominant R wave in V1 and V2 with ST segment depression, suggestive of posterior ST-elevation myocardial infarction.
This is one STEMI where you may not find distinct ST-segment elevation but still is considered and treated like a STEMI. It is usually but not always associated with inferior ST segment elevation. In case of doubt, use posterior leads, for example, V7-9 to bring out the ST elevation. Angiographically, it is associated with left circumflex territory infarct and if the patient suddenly becomes short of breath and not able to lie down flat, always consider papillary muscle rupture, usually posteromedial, as it has single source of blood supply.
Clinically, you may not hear the mitral regurgitation murmur due to equalization of LV and LA pressures and echocardiography may not pick up this mechanical complication or underestimate its severity. LV angiography usually brings out the presence and severity of mitral regurgitation due to papillary muscle rupture.
Whether you got the question right or wrong, our upcoming webinar will provide you with valuable insights to make sure you're well equipped to provide the best care for patients with STEMI.
Challenges in EKG Interpretation in Patients with STEMI Webinar
June 10, 2020
10 - 11 a.m. CDT
Cost: Free
- Discuss the EKG diagnosis of STEMI
- Identify angiographic correlation of STEMI
- Discuss pitfalls and helpful hints to improve your diagnosis
- Review the differential diagnosis of STEMI